![[ Click Here to Enter an Alternate Text for this Image ]](/data//sites/default/files/report_2387/images/image_file_0_FirstPageImage_1112020842.jpg)
- Based on combined 2013–2014 National Surveys on Drug Use and Health, 2.6 million young adults aged 18 to 25 in the United States had serious thoughts of suicide in the past year.
- Based on combined 2013–2014 National Surveys on Drug Use and Health, about 1 in 13 young adults had suicidal thoughts in the past year.
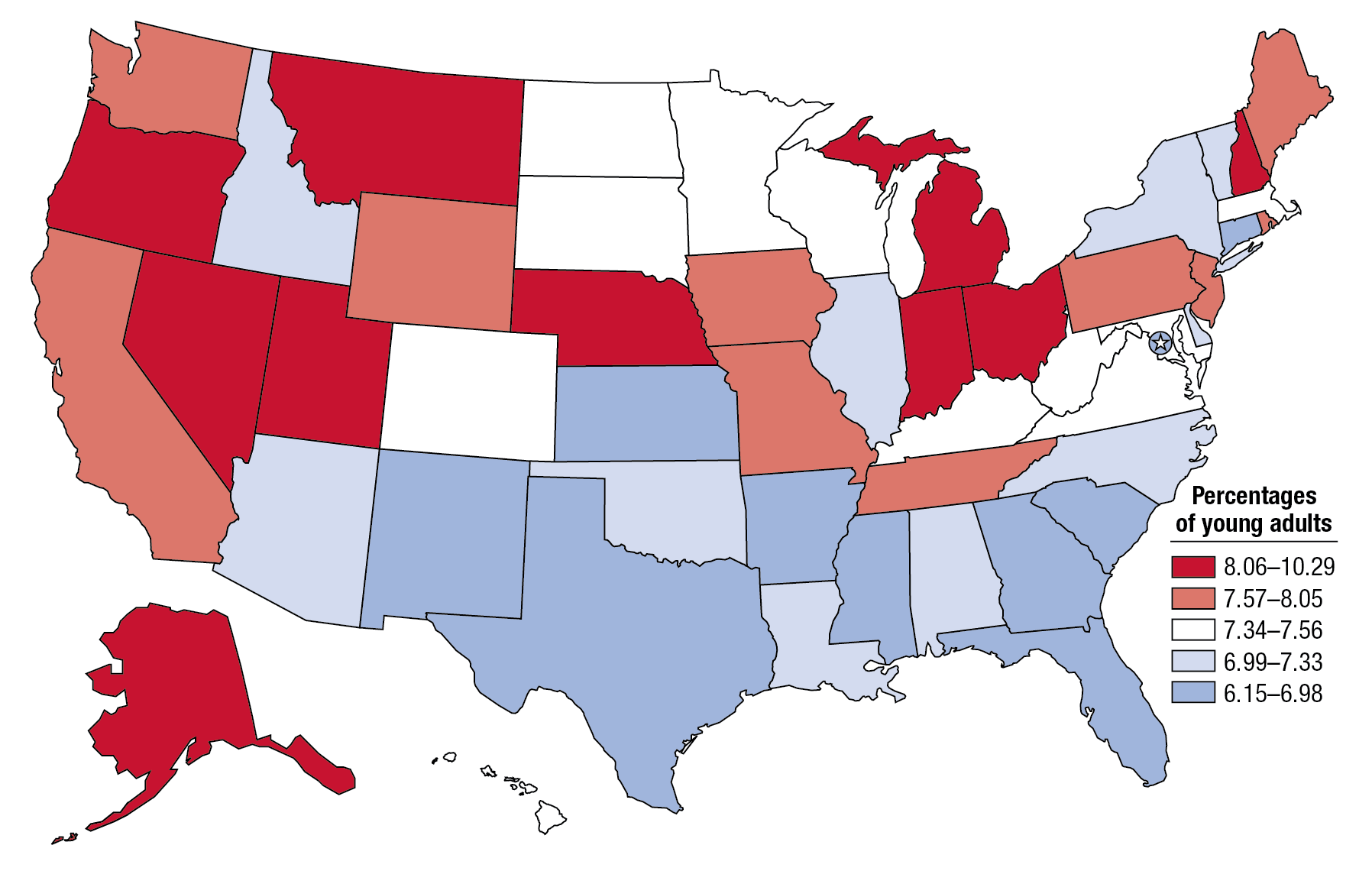
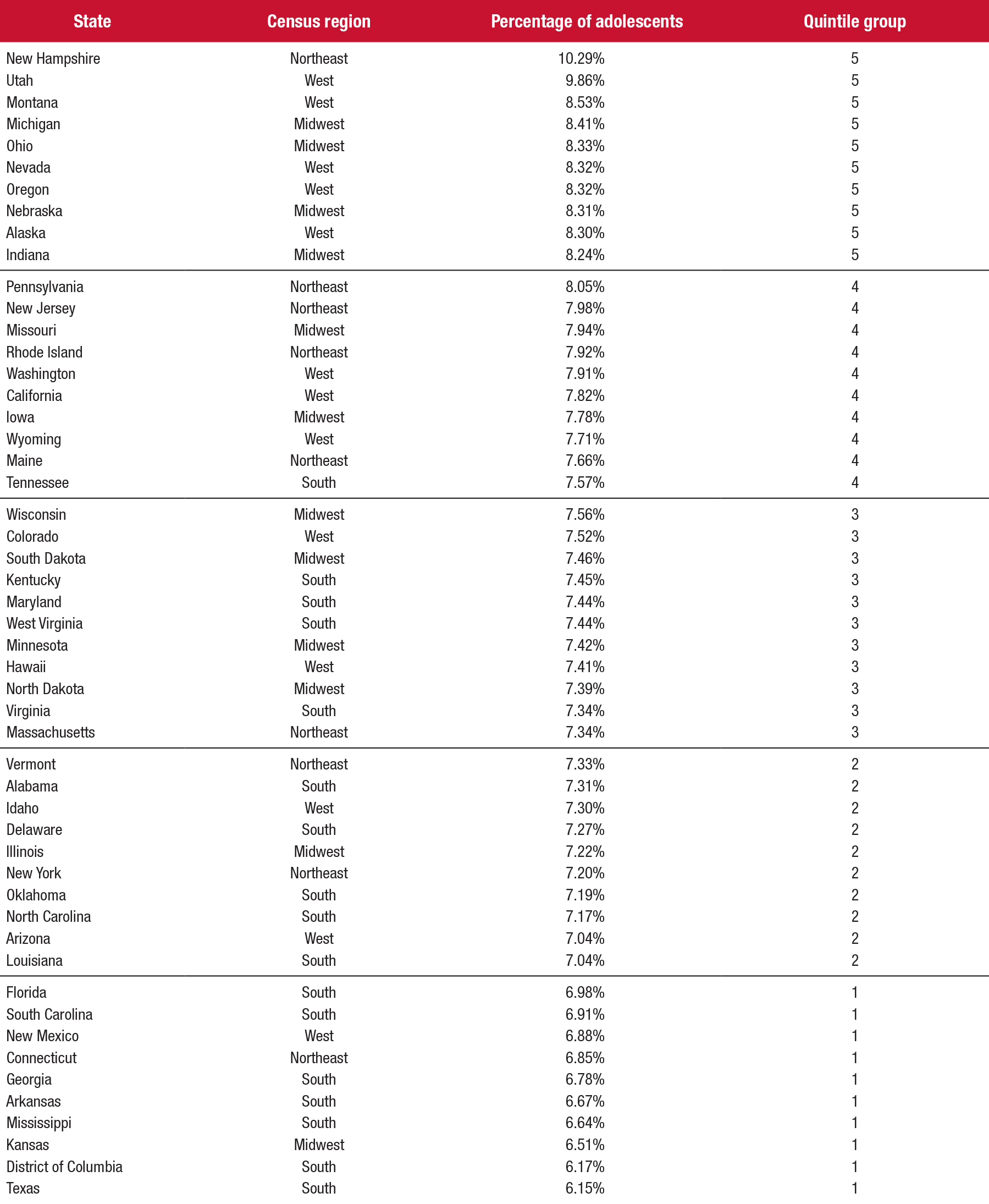
- Past year serious thoughts of suicide among young adults ranged from 6.2 percent in Texas to 10.3 percent in New Hampshire.
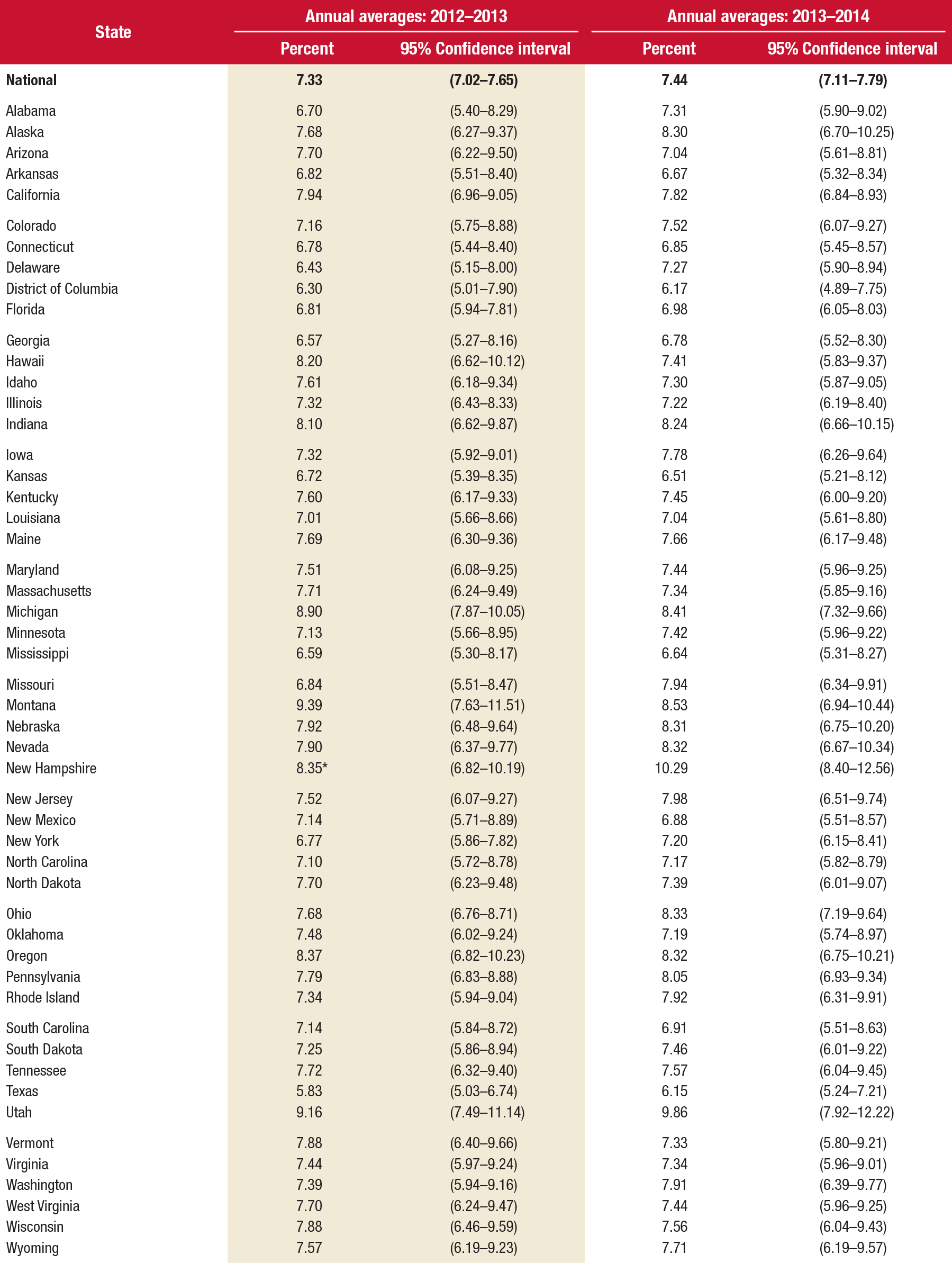
- The prevalence of past year serious thoughts of suicide increased in New Hampshire (when comparing 2013–2014 estimates with 2012–2013 estimates) but remained unchanged in 49 states and the District of Columbia.
Suicide is an avoidable cause of mortality that is a tragedy for all involved—families, friends, neighbors, colleagues, and communities. In 2013, suicide was the 10th leading cause of death in the United States overall, with more than 41,000 deaths by suicide.1 Among people aged 15 to 24, suicide ranked even higher as the second leading cause of death.2
However, individuals who die from suicide represent a fraction of those who consider or attempt suicide. Research suggests that there are more attempted suicides than there are deaths from suicide.3,4 Out of every 31 adults who attempted suicide in the past 12 months in the United States, there was 1 death by suicide.5 In addition, people are likely to have thought about suicide before actually attempting suicide. Suicide is of particular concern for young adults because the percentage of adults having serious thoughts of suicide in 2014 was higher among young adults aged 18 to 25 than among adults aged 26 to 49 and adults aged 50 or older (7.5 percent vs. 4.0 and 2.7 percent, respectively).6 Assessing recent state-level trends in past year serious thoughts of suicide among young adults helps state public health authorities and suicide prevention specialists to better understand and effectively serve their communities.
The National Survey on Drug Use and Health (NSDUH) has information on suicidal thoughts and behavior at the state level. This issue of The CBHSQ Report uses data from the 2013 and 2014 NSDUHs to present state (including the District of Columbia) estimates of serious thoughts of suicide in the past year among adults aged 18 to 25. The estimates in this report do not reflect information from adults whose suicide attempts in the past year were fatal. All estimates in this report are based on a small area estimation (SAE) methodology in which state-level NSDUH data are combined with local-area county and census block group/tract-level data from the state to provide more precise estimates.7 Findings in this report are annual averages based on combined 2013–2014 NSDUH data from 39,000 adults aged 18 to 25. The 2012 and 2013 data are based on information obtained from 45,200 young adults.8