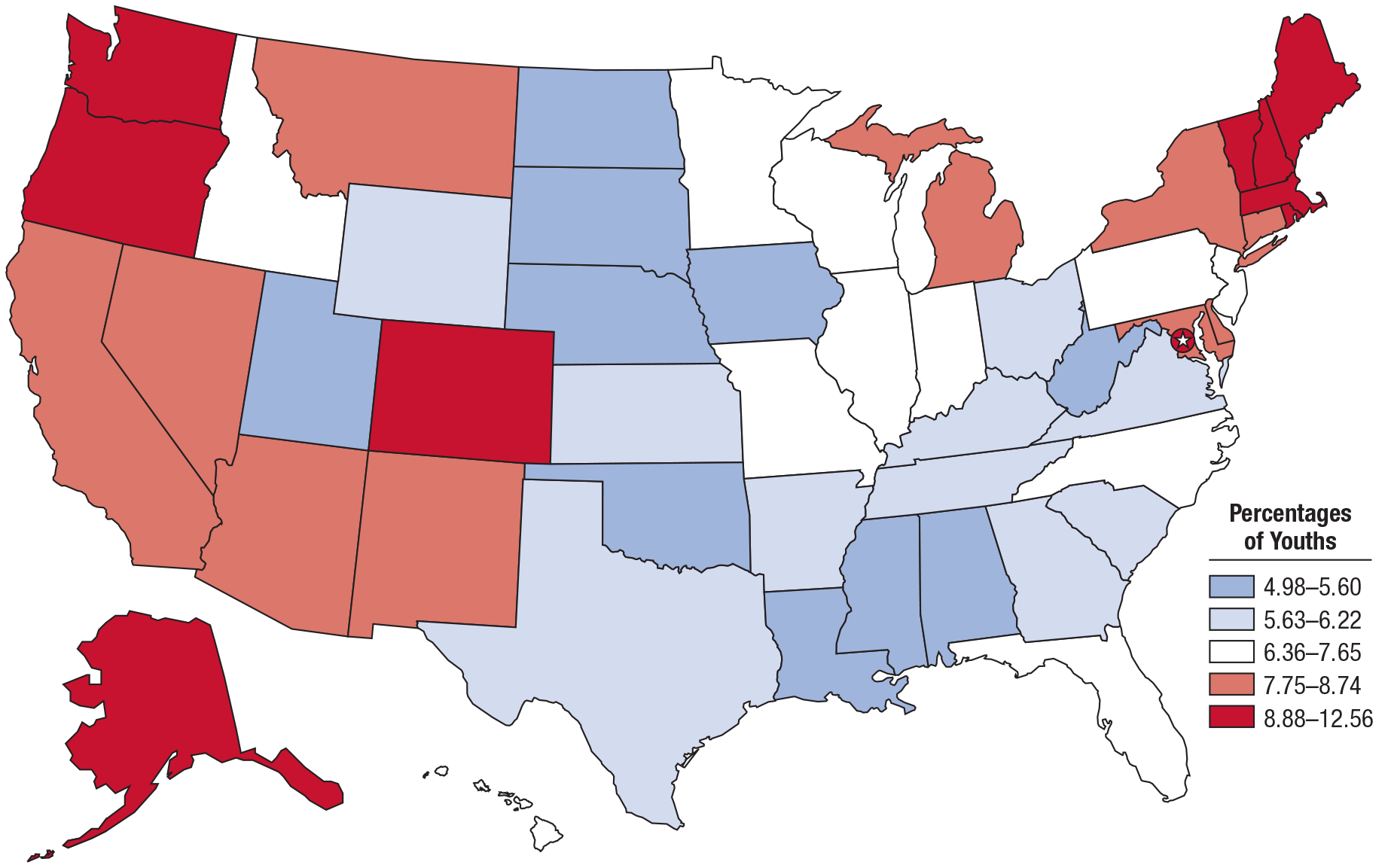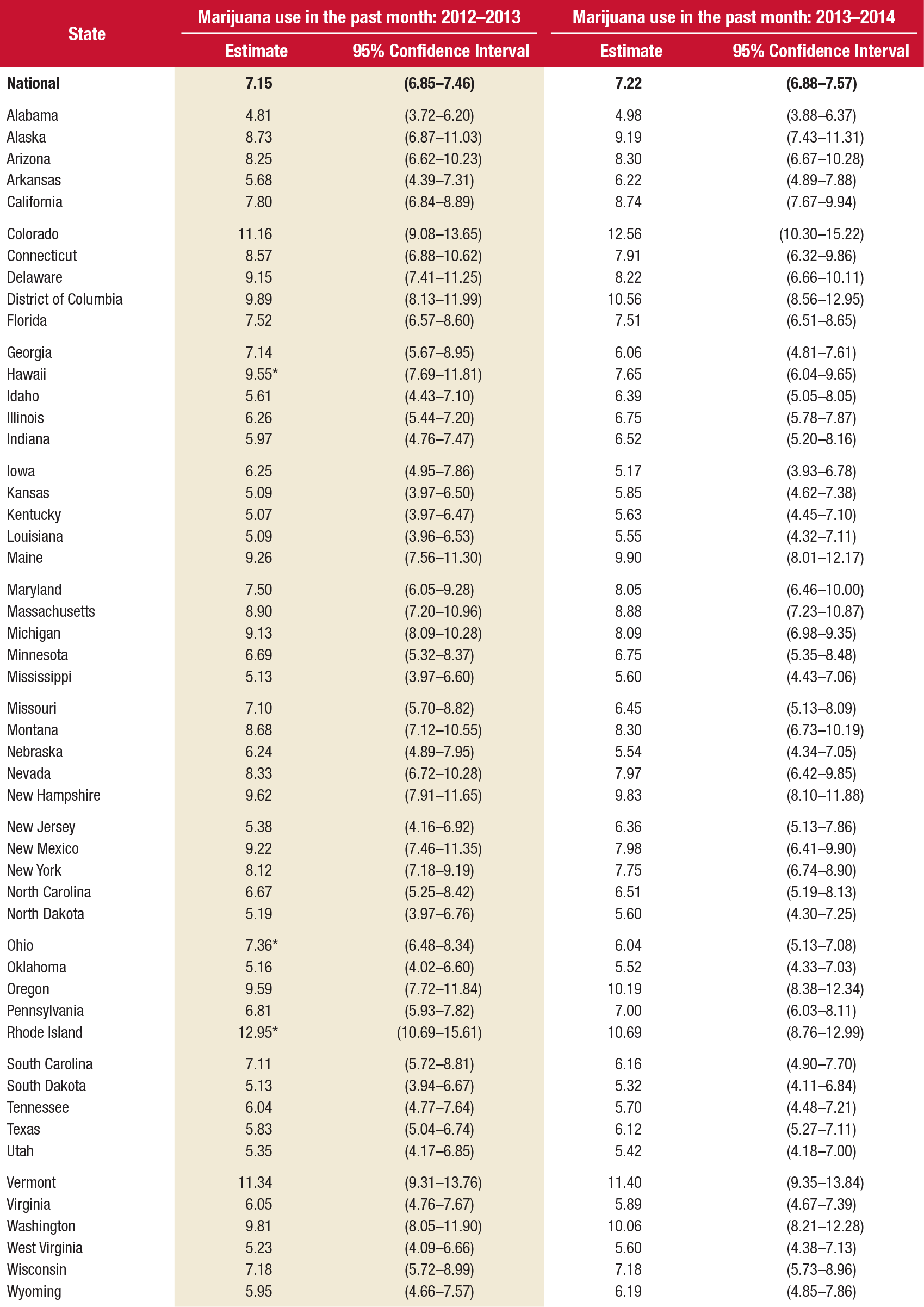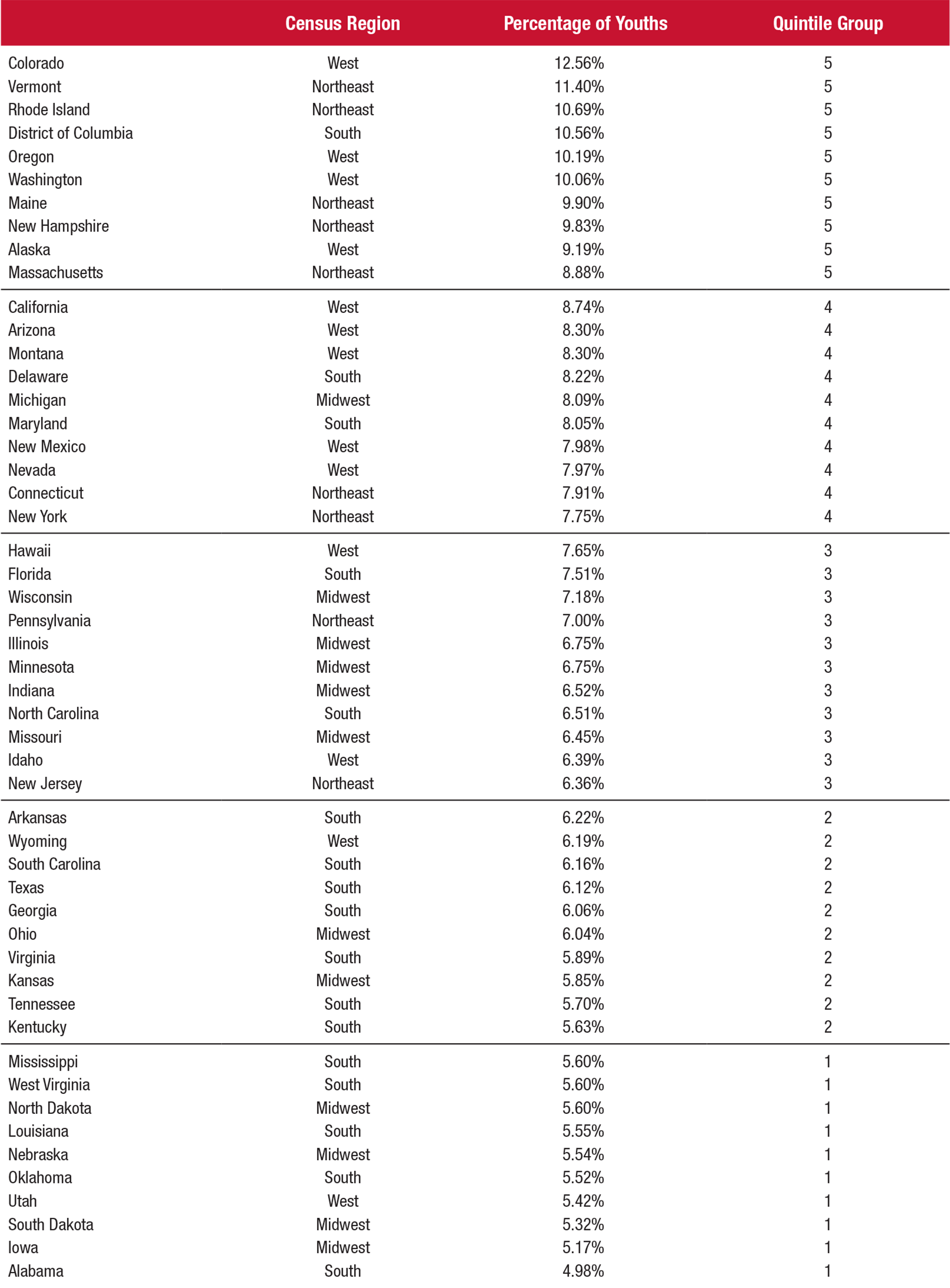
- Based on 2013-2014 data, 7.22 percent of adolescents aged 12 to 17 across the nation used marijuana in the past month. Adolescent marijuana use ranged from 4.98 percent in Alabama to 12.56 percent in Colorado.
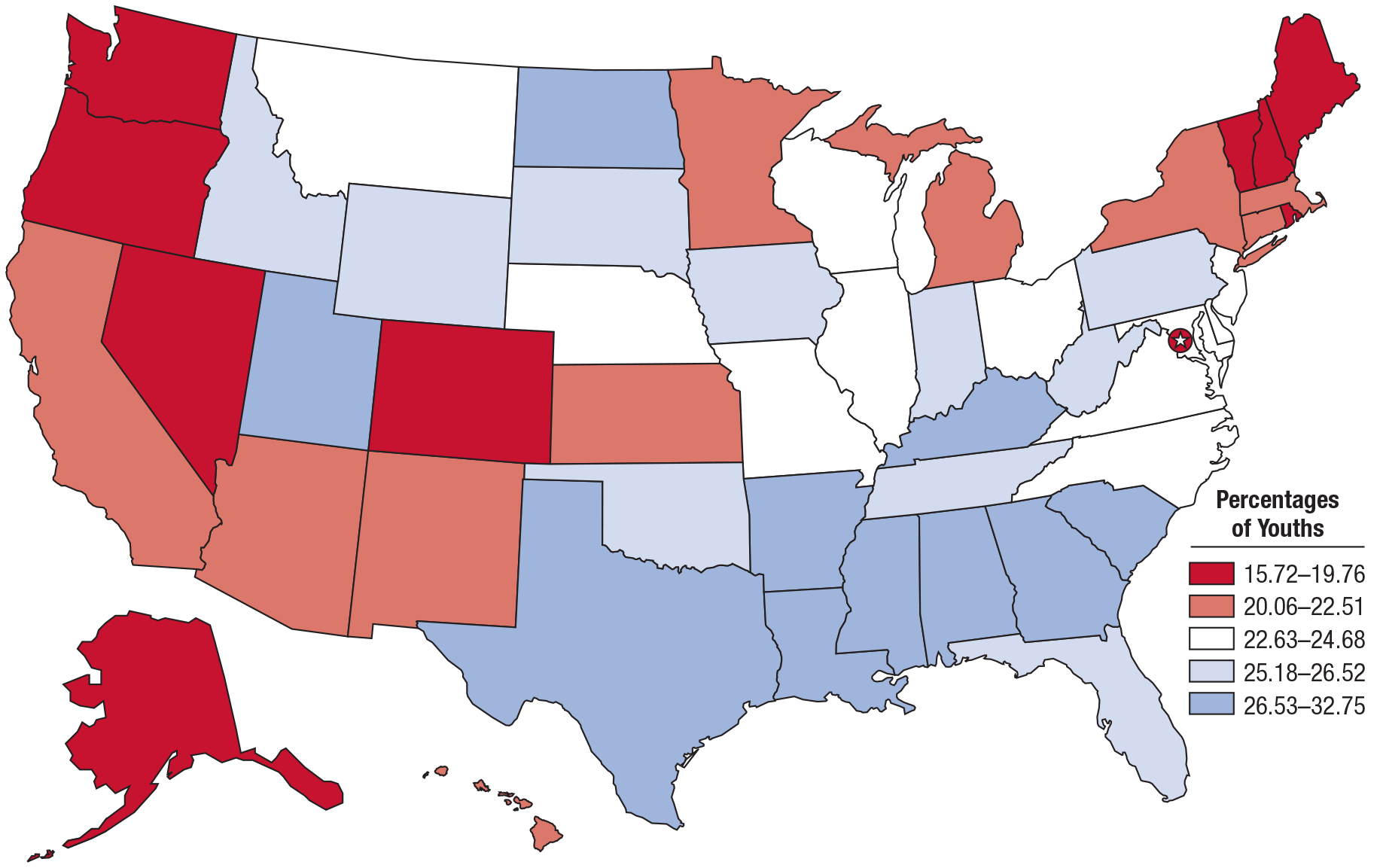
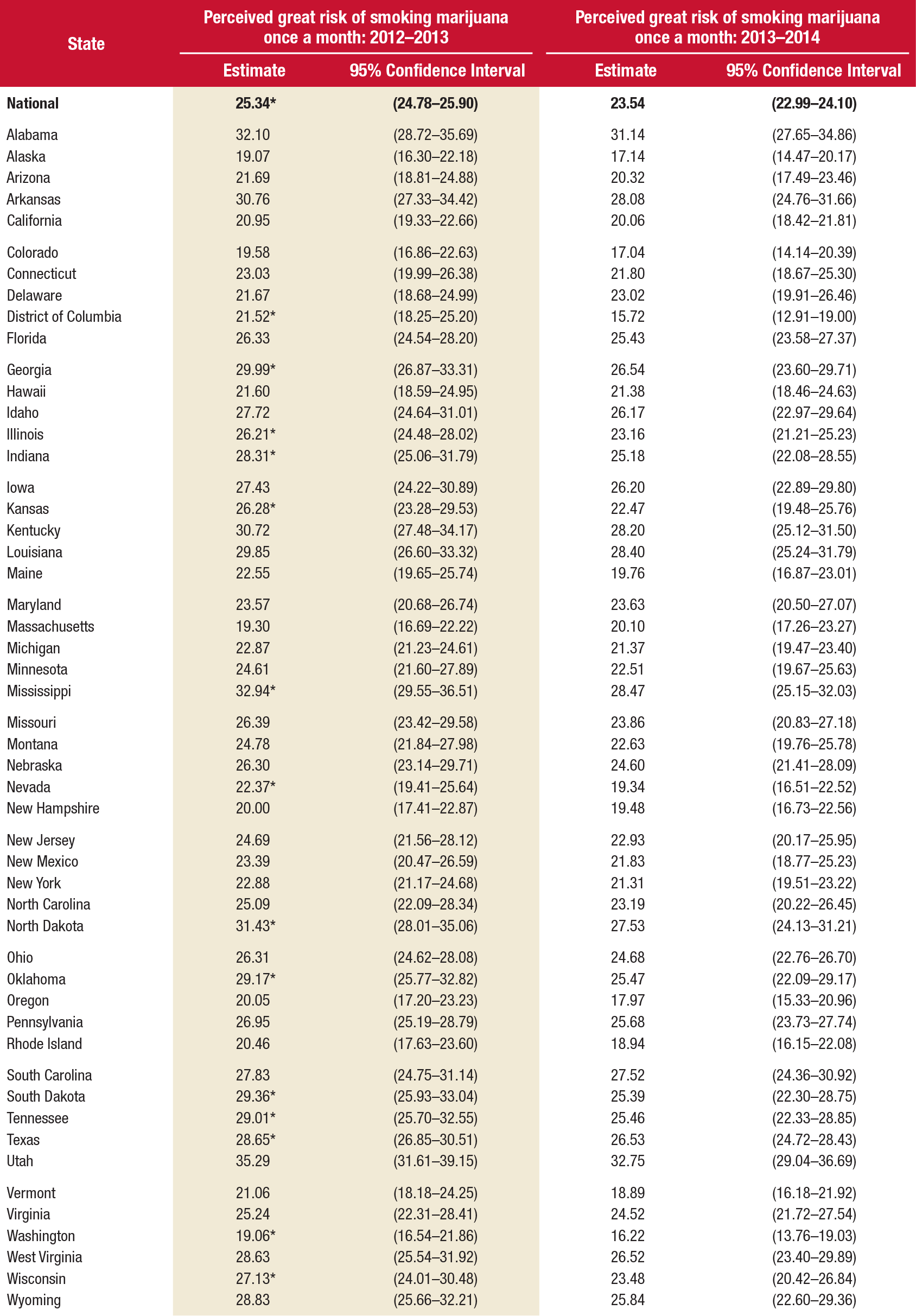
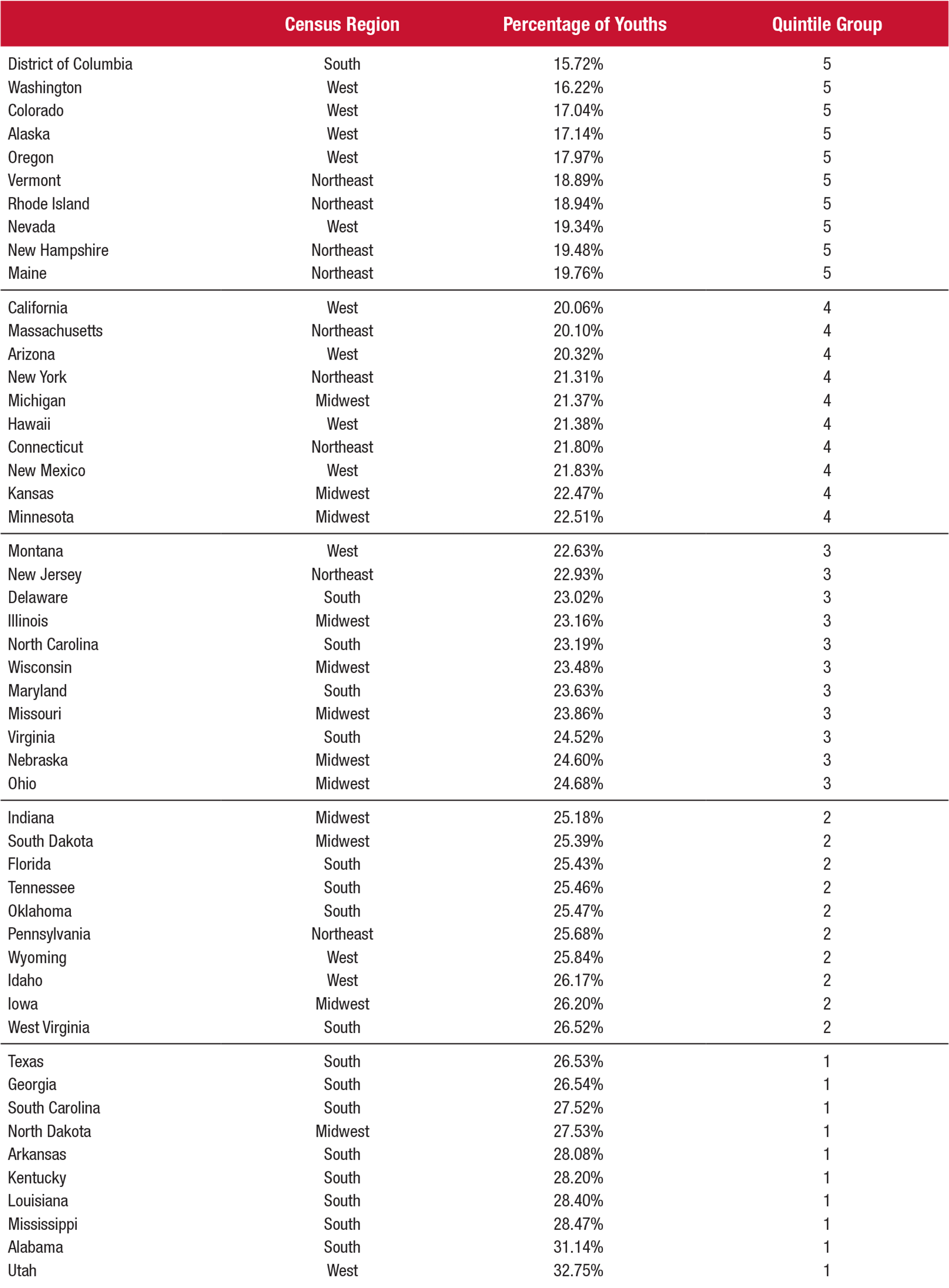
- In 2013–2014, about one out of four (23.54 percent) adolescents nationwide perceived great risk in smoking marijuana once a month (i.e., monthly use), ranging from 15.72 percent in the District of Columbia to 32.75 percent in Utah.
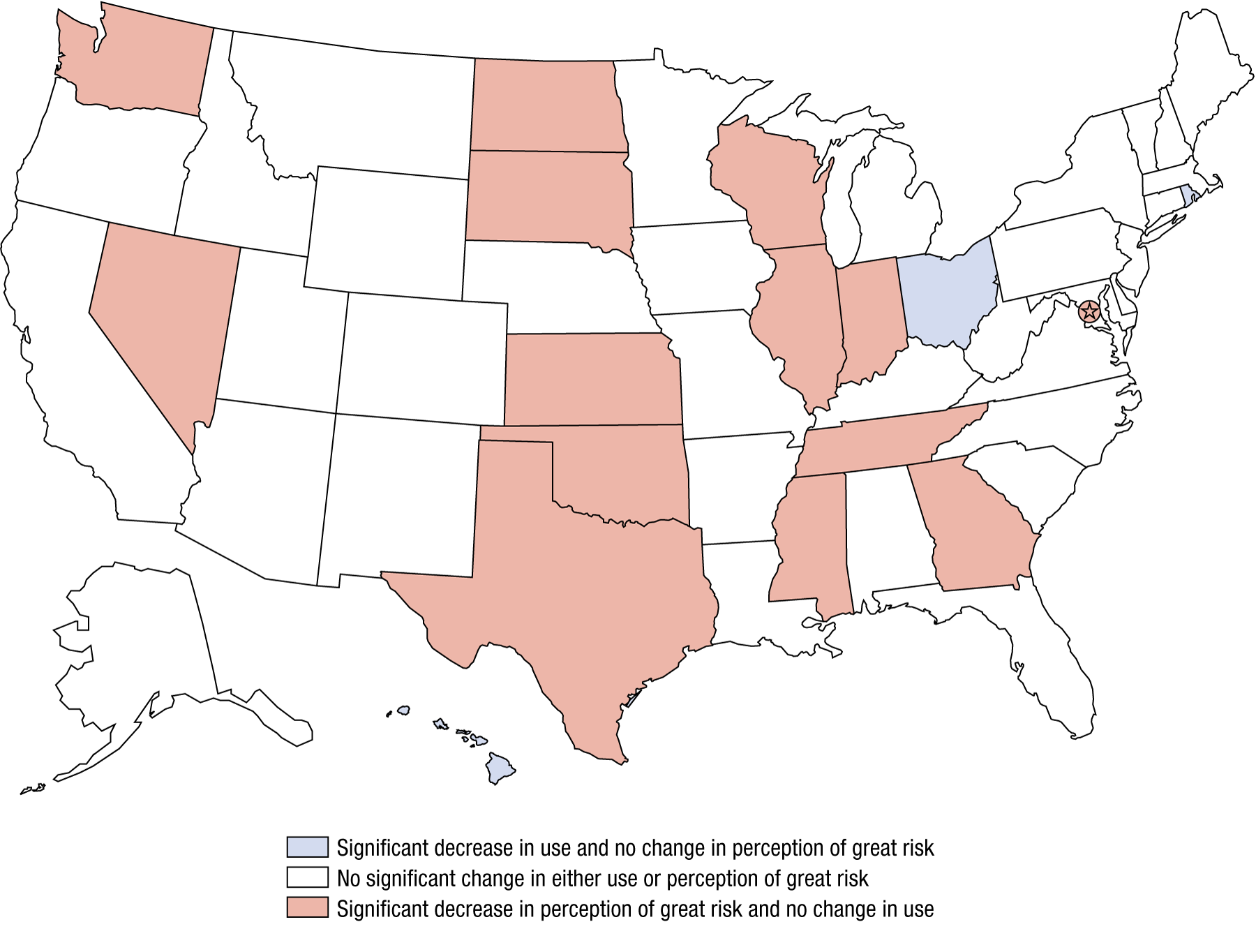
- Adolescent marijuana use remained unchanged in 48 states and declined in 3 (comparing 2013–2014 estimates to 2012–2013 estimates). However, youth perceptions of great risk of harm from monthly marijuana use decreased in 14 states, while 37 states experienced no change.
Marijuana is the most commonly used illicit drug in the United States for the population overall and for youths in particular.1 Although the laws regarding marijuana use have changed in a number of states over the past decade, marijuana use remains illegal under federal laws in all states (e.g., the Controlled Substances Act; http://www.fda.gov/regulatoryinformation/legislation/ucm148726.htm).
Research has indicated that there are health risks associated with youth marijuana use,2 including poorer education/employment outcomes,3 poorer cognitive outcomes,4,5 increased likelihood of vehicle crashes,6 and increased addiction risk.7 Even though research indicates that youth marijuana use is a health risk, nationally only 1 in 5 adolescents perceived great risk from monthly marijuana use in 2014, which is lower than in any other year from 2002 to 2013.8 Preventing adolescents from starting to use marijuana is an effective way to reduce the impact of marijuana use in the future. Thus, it is useful for state policymakers and prevention specialists to assess recent trends in youths' marijuana use and their perception of the great risk of harm to their health from marijuana use.
All states continue efforts to reduce adolescent marijuana use. As longitudinal research has shown, youth attitudes about the risks associated with substance use are often closely related to their use, with an inverse association between use and risk perceptions (i.e., the prevalence of use is lower among those who perceive high risk of harm from use).9 Thus, states with a high prevalence of adolescent marijuana use would be expected to have a low prevalence of adolescent perception that there is a great health risk from using marijuana. State-level information about marijuana use and attitudes about marijuana use can provide states with vital data to inform educational and prevention efforts.
This issue of The CBHSQ Report uses National Surveys on Drug Use and Health (NSDUH) data to present national and state (including the District of Columbia) estimates of past month marijuana use and perceptions of great risk from smoking marijuana once a month among youths aged 12 to 17.10 Estimates are annual averages based on combined 2013 and 2014 NSDUH data from 39,600 respondents.10 The combined 2013-2014 estimates are compared to estimates from combined 2012-2013 data, which are based on responses from 45,000 youths aged 12 to 17.11