
Background: Nationwide, there is concern about challenges in the retention of the behavioral health workforce, which includes mental health services. Members of the mental health treatment workforce benefit from continued training and clinical supervision to maintain high-quality services and prevent emotional exhaustion, burnout, and turnover. Mental health treatment facilities can play a key role in supporting their workforce through training and supervision practices. Method: Data from the 2010 National Mental Health Services Survey (N-MHSS) were used to examine the percentage of facilities that used quality assurance practices related to the behavioral health workforce and whether the percentage of facilities differed based on facility characteristics and by U.S. state (as evidenced by Cohen's h effect size ≥0.20). Results: Most facilities (89.4 percent) monitored the continuing education requirements for professional staff. Almost all facilities (91.5 percent) had regularly scheduled case review with a supervisor, and many facilities (70.3 percent) had regularly scheduled case review by an appointed quality review committee; only 4.9 percent of facilities used neither type of case review practice. States differed in the use of quality assurance practices. Conclusion: Given that quality assurance practices related to the behavioral health workforce are common standard operating procedures in mental health treatment facilities, opportunities to enhance the quality of the practices should be supported.
Keywords: Behavioral health workforce, mental health treatment, mental health services, continuing education, clinical supervision, case review, training
Behavioral Health Workforce: Quality Assurance Practices in Mental Health Treatment Facilities (Test Report)

Data Sources National Mental Health Services Survey
Please choose an item for download
Select then copy text below to cite this report
Sherman, L. J., Lynch, S. E., Greeno, C. G. and Hoeffel, E. M. Behavioral health workforce: Quality assurance practices in mental health treatment facilities. The CBHSQ Report: July 11, 2017. Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, Rockville, MD.
Downloads
Summary
N-MHSS, conducted by SAMHSA, is an annual7 survey of all known public and private mental health treatment facilities in the United States. N-MHSS is the only source of national and state-level data on the mental health services reported by publicly and privately operated specialty mental health treatment facilities. N-MHSS is used to collect basic data on the number, location, and characteristics of specialty mental health treatment facilities and the people they serve throughout the 50 states, the District of Columbia, and other U.S. jurisdictions.8 N-MHSS is a point-prevalence survey that provides a picture of facilities' activities on a typical day but may not represent the full scope of practice in a given year.
The 2010 N-MHSS data are used for this report.9,10 There were 10,374 eligible mental health treatment facilities that responded to the survey. The response rate was 91.2 percent. Basic facility information, service characteristics, and client counts were reported for 9,139 of the 10,374 facilities. This report examines use of three types of quality assurance practices: (1) monitoring continuing education requirements for professional staff, (2) regularly scheduled case review with a supervisor, and (3) regularly scheduled case review by an appointed quality review committee. There was some missing data for each quality assurance practice; the numbers of facilities reporting data for each practice were 9,117, 9,116, and 9,101, respectively. There was also some missing data for facility characteristics (facility operation and service delivery setting). The percentages described in this report were calculated using available data for each analysis presented, and the totals used to calculate the percentages are listed in the tables.
Because N-MHSS is considered a census of facilities and provides actual counts rather than estimates, statistical significance and confidence intervals are not applicable. The differences between percentages mentioned in this report were assessed using Cohen's h. The results described here have a Cohen's h effect size ≥0.20, which indicates that there were meaningful differences between the groups.11

In 2010, quality assurance practices related to the behavioral health workforce were common standard operating procedures in mental health treatment facilities. Specifically, 89.4 percent of mental health treatment facilities monitored continuing education requirements for professional staff as a standard operating procedure; 91.5 percent of mental health treatment facilities used regularly scheduled case review with a supervisor as a standard operating procedure; and 70.3 percent of mental health facilities used regularly scheduled case review by an appointed quality review committee as a standard operating procedure (Figure 1).
The percentage of mental health treatment facilities that monitored the continuing education requirements for professional staff did not vary by type of facility operation with one exception (Table 1). Specifically, facilities operated by the U.S. Department of Veterans Affairs (VA) had a higher percentage of facilities monitoring continuing education requirements for professional staff as a standard operating procedure than the U.S. percentage overall (98.2 vs. 89.4 percent).
The percent of mental health treatment facilities that used regularly scheduled case review with a supervisor as a standard operating procedure varied. Compared with the U.S. percentage overall, a smaller percentage of facilities operated by a regional or district authority and by the VA used this practice (79.9 and 78.3 vs. 91.5 percent, respectively; Table 1).
The percent of mental health treatment facilities that used regularly scheduled case review by an appointed quality review committee as a standard operating procedure varied. Compared with the U.S. percentage overall, a lower percentage of facilities operated by a regional or district authority used this practice (55.9 vs. 70.3 percent), whereas a higher percentage of facilities operated by the VA used this practice (79.6 percent).
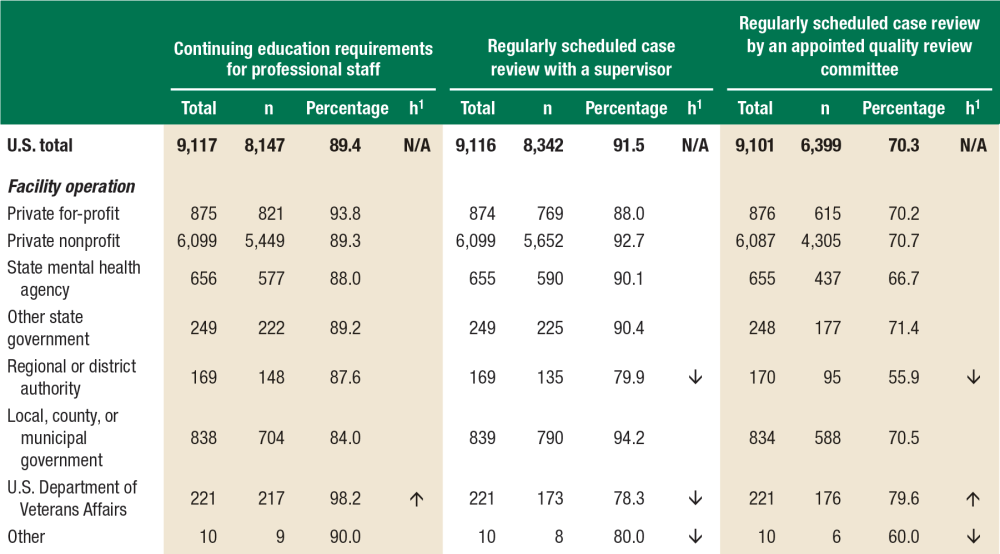
Note: Totals vary across quality assurance practices because of missing data.
Source: SAMHSA, Center for Behavioral Health Statistics and Quality, National Mental Health Services Survey (N-MHSS), 2010.
A higher percentage of facilities offering inpatient services monitored continuing education for professional staff compared with the U.S. percentage overall (95.4 vs. 89.4 percent), whereas facilities that offered outpatient or residential settings were not different from the U.S. percentage (89.3 and 87.7 percent, respectively) (Table 2). It should be noted that these service delivery settings were not mutually exclusive; thus, some facilities offered services in two or more settings.
A lower percentage of facilities offering inpatient services used case review with a supervisor as a standard operating procedure compared with the U.S. percentage (79.5 vs. 91.5 percent), whereas facilities offering services in outpatient and residential settings were not different from the U.S. percentage (93.1 and 94.6 percent, respectively; Table 2).
The percentage of facilities using case review by an appointed quality review committee as a standard operating procedure did not vary by service delivery setting (Table 2).
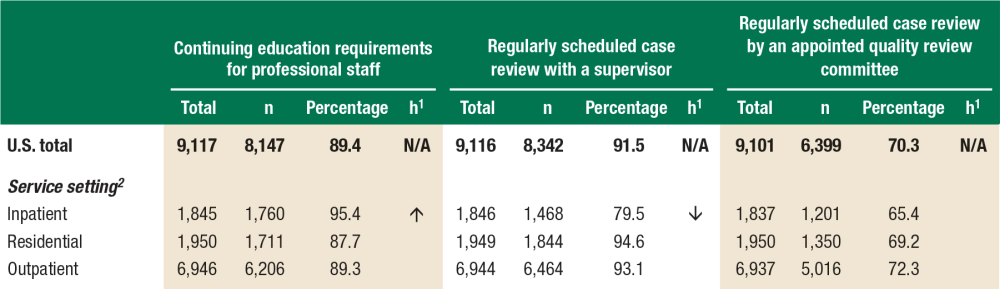
2 Service settings were not mutually exclusive; thus, some facilities offered services in two or more settings.
Note: Totals vary across quality assurance practices because of missing data.
Source: SAMHSA, Center for Behavioral Health Statistics and Quality, National Mental Health Services Survey (N-MHSS), 2010.
The majority of facilities (66.8 percent) used both types of case review practices as standard operating procedures (regularly scheduled case review with a supervisor and regularly scheduled case review by an appointed quality review committee; Figure 2). The next most common pattern (24.8 percent) was for facilities to use regularly scheduled case review with a supervisor as a standard operating procedure but not case review by an appointed quality review committee. The least common pattern (3.6 percent) was for facilities to use case review by an appointed quality review committee but not case review with a supervisor. The remaining 4.9 percent of facilities used neither case review practice as a standard operating procedure.

States varied in their use of the three quality assurance practices examined in this report (Table 3). Delaware was the only state with a higher percentage of facilities using all three practices compared with the percentage for the United States overall.
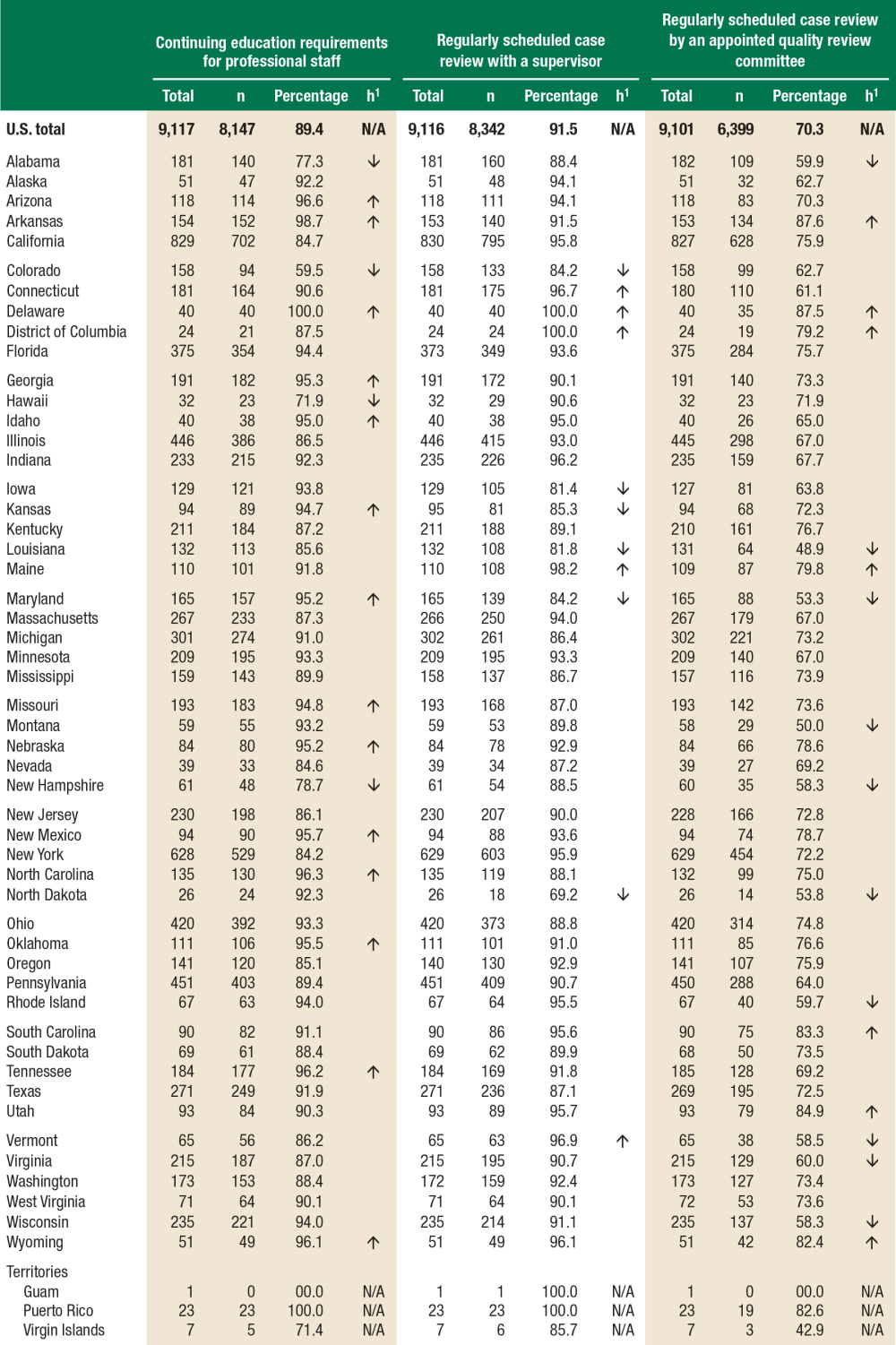
Source: SAMHSA, Center for Behavioral Health Statistics and Quality, N-MHSS 2010.
The 2010 N-MHSS data used in this report indicate that quality assurance practices related to the behavioral health workforce are common in mental health treatment facilities. Regularly scheduled case review with a supervisor was the most commonly used practice, followed closely by monitoring continuing education requirements for professional staff. Although regularly scheduled case review by an appointed quality review committee was a less commonly used standard operating procedure than review with a supervisor or monitoring continuing education requirements, it was still common in facilities. About two thirds of facilities used both types of case review in their standard operating procedures. Facilities operated by a regional or district authority had lower percentages of both types of case review when compared with the U.S. total. Although compared with the other settings, facilities offering inpatient services had higher percentages of monitoring continuing education requirements for professional staff and lower percentages of regularly scheduled case review with a supervisor as standard operating procedures.
Facilities can play a role in supporting the behavioral health workforce by including the practices outlined in this report in their standard operating procedures.1,2 The best quality outcomes are likely to be produced when they go beyond the provision of basic continuing education and clinical supervision.12,13 For example, continuing education that is interactive or tailored to individuals' practices and clinical supervisor expertise, especially in the areas of competencies and procedural knowledge, tends to yield better outcomes.12,13,14 Furthermore, studies indicate that formal documentation and evaluation are important when supervision is conducted in groups,15 which has implications for case review by a quality review committee. Some practices may be more easily integrated into existing facility procedures, such as monitoring the continuing education requirements for professional staff, compared with other practices that require greater time, resources, coordination, and funds (e.g., case review by a quality review committee). Online tools, video conferencing, and electronic health records might facilitate case review for facilities in understaffed or under-resourced areas.16,17 Additional resources to support the behavioral health workforce can be found at http://www.samhsa.gov/workforce and http://www.integration.samhsa.gov/workforce/education-training.
Did You Know?
![]()
SAMHDA provides public use data to support a better understanding of substance abuse and mental health. See how.